Behavioural addictions, also known as process addictions (Grigsby, 2020), are a growing area of research. While their definition may vary, they typically refer to behaviours which do not involve substance use but do involve diminished control over the impulse to engage in certain behaviours and a failure to cut down or give them up despite adverse consequences, including damaging oneself or others (Grant et al., 2010; Griffiths, 2000; Potenza, 2006; Wareham & Potenza, 2010). Behavioural addictions can include a wide range of behaviours including internet use, relationships and sex, shopping, and gambling. There are various estimations for the prevalence of behavioural addictions in the general population, with an estimated 1%–2% for gambling, 5% for sex and relationships, less than 1% for internet addictions (6% among internet users), 1%–6% for buying addictions, and 3% for eating addictions, and while there are no epidemiological studies on work addictions, some claim that it is as high as 25% of the working population (Freimuth et al., 2008).
The majority of research on behavioural addictions has focused on nosology and definitions (i.e., whether behavioural addictions fit under impulse control or compulsions; Grant et al., 2010), prevalence, co–occurrence with other addictions (both behavioural and substance), or correlation with mental health conditions such as depression, anxiety, personality disorders, and phobias (Freimuth et al., 2008). While some research on parenting and the risk of developing behavioural addictions in adulthood has been carried out (e.g., examining the link between an affectionless control parenting style and behavioural addictions; Grant & Kim, 2002; Siomos et al., 2012; Villalta et al., 2015), very little research has studied the long-term impact of growing up with a parent/s with behavioural addictions. There is not yet a sufficient body of work on behavioural addictions, but the small number of studies available suggest a long–term adverse effect of parental behavioural addictions (see e.g., McPherson et al., 2013).
Due to the scarcity of research in the area of behavioural addictions, we turn to the well–documented long–term impact of parental substance addictions (e.g., Barrocas et al., 2016; Corbett, 2005; Hill et al., 1996). Children of parents with substance addictions reveal higher levels of antisocial behaviours, depression, anxiety, low self–esteem, substance abuse and eating disorders (Arria et al., 2012; Biederman et al., 2000; Forrester & Harwin, 2006, 2008; Fraser et al., 2009; Hussong et al., 2005; Velleman & Templeton, 2016). In terms of the long–term impact of parental substance addictions, it seems that children of parents with substance addictions are at a higher risk of developing substance abuse and other mental health conditions in adulthood (Catalano et al., 2002). Some suggest that this impact is due to harmful interactions with parents who are “under the influence” (Corbett, 2005; Hill et al., 1996) while others argue that it is not the intoxication itself that causes harm but rather a family dysfunction caused by addiction, referring to instances such as a child worrying constantly about the parent, being forced to take sides between conflicting parents, being subjected to unpredictable behaviours, or lack of consistency, guidelines or structure (Barrocas et al., 2016).
Indeed, previous findings suggest that a disruptive family environment can be exacerbated by addiction–related circumstances such as parental illegal behaviours (consumption–related), legal proceedings, financial problems leading to a stressful and unpredictable environment (e.g., Barnard, 2007; Catalano et al., 2002; Keller et al., 2002) and parental neglect (Testa & Smith, 2009). While most of the work in the area has focused on substance addictions, some studies have identified various behavioural addictions which can lead to stressful circumstances similar to those found in substance abuse e.g., gambling and shopping addictions (Ledgerwood et al., 2007; Villella et al., 2011) and relationship addictions (Grant et al., 2010). It should be noted, however, that unlike substance addictions, behavioural addictions are mostly hidden and often undiagnosed (Freimuth, 2009) and parents with such addictions are less likely to receive help or support both in terms of managing their addiction and the impact on their family (Engel et al., 2012; Manthorpe et al., 2018).
According to Dvir et al. (2014), in such disruptive family environments children internalise negative experiences which results in long-term symptoms including dissociation, depression and addiction. This implies that family dysfunction may have a mediating effect on the relationship between parental addictions and have a negative long-term impact on mental health. Other studies on families with substance addictions have indicated a link between parental practices and children’s psychological resilience (for a review, see Armstrong et al., 2005). Finally, Leys et al. (2017) found a full mediating effect for psychological resilience on the well-documented relationship between family dysfunction and children’s mental health in adulthood. The current study will examine a similar mediating path albeit in the context of parental behavioural addictions.
Psychological resilience refers to one’s ability to minimise negative outcomes when exposed to adversity or risk (Garmezy, 1991; Lee & Cranford, 2008; Masten, 2001; Rutter, 1990), or to recover or even grow from adversity (Leipold & Greve, 2009). Psychological resilience can be seen as a trait, (i.e., a stable personal consolation/personality quality; Block & Block, 1980; Connor & Davidson, 2003) or as a process that changes according to circumstances (Luthar et al., 2000). In the context of addictions, Park and Schepp (2015), in a systematic review of children of alcoholic parents, considered children’s vulnerability and psychological resilience on four levels: the individual level (e.g., age, gender, cognitive and academic abilities, temperament, self regulation and self–esteem), the parental level (e.g., attachment style, parent–child relationship, parentification), the familial level (e.g., family violence, family cohesion, trusted family members and parents’ co–morbid mental health conditions), and the social level (e.g., social support, extra–curricular activities, positive relationships later in life). In studies related to addictions, several aspects of family dynamics/environments were found to promote psychological resilience including direct involvement and clear communication (e.g., Wyman et al., 2000), family cohesion and family adaptability (Leys et al., 2017; Moriarty et al., 2011), effective disciplining, and consistency (Armstrong et al., 2005). Other factors such as hostility, rejection, control and neglect (Lind et al., 2018) as well as invalidation and inconsistent discipline (Hann & Borek, 2001), were linked to reduced levels of psychological resilience.
The Present Study
The aim of this study was to examine the role that a disruptive family environment and individual psychological resilience play in the relationship between having a parent who is perceived to have had behavioural addictions (retrospectively identified by participants), and individual mental health in adulthood. Taking together various findings on the long-term impact that parental addiction has on children (e.g., Catalano et al., 2002; McPherson et al., 2013), the link between addictions and disruptive family environments (e.g., Barnard, 2007; Catalano et al., 2002; Keller et al., 2002; Testa & Smith, 2009), the link between family dynamics and psychological resilience (e.g. Armstrong et al., 2005; Leys et al., 2017; Moriarty et al., 2011; Wyman et al., 2000), and Leys et al.'s (2017) study which found that psychological resilience fully mediated the link between family dynamics and mental health, we predict that the link between parental behavioural addictions and mental health will be mediated by a disruptive family environment which will be linked to reduced psychological resilience and then to reduced mental health . Based on these findings, we hypothesise that:
-
Participants who report having parents with behavioural addictions will show higher levels of substance and behaviour dependence and lower levels of mental health than those who report having parents with no addictions.
-
Participants who report having parents with behavioural addictions will have a more disruptive family environment than those who report having parents with no addictions.
-
The level of disruption to the family environment during childhood and psychological resilience will mediate the relationship between parental behavioural addictions and participants’ mental health.
-
The level of disruption to the family environment during childhood and psychological resilience will mediate the relationship between parental behavioural addictions and participants’ own substance and behaviour dependency.
Methodology
Participants and Procedure
The project was approved by Goldsmiths, University of London, ethics committee. Information that included the aims of the study, participation, confidentiality and contact for potential complaints appeared on the survey’s front page. Participants then ticked a box confirming that they have read the information and are 18 or older before being directed to the online. Participation was voluntary and anonymous.
Our sample included respondents to an online survey. Overall 607 people visited the survey which was published on a specific website via the link “www.substancevsprocess.com” and advertised both on social media (e.g., Facebook), specific websites for people with addictions, and through visiting cards distributed randomly to the general public in central London, UK. Out of the 607 people who visited the survey, 292 (48%) completed it. The mean age of the sample was 32.86 (SD = 12.37), 76.1% were women, 22.9% were married, and the majority (84.9%) identified themselves as White while out of all other participants, 3.5% identified as Asian/South Asian (including, India, Bangladeshi and Pakistani), 2.4% as African, 2.8% as mixed race, 1.7% as Caribbean, 1.4% as Chinese, and 3.3% did not wish to disclose their ethnicity. Socio-economic level was measured through annual household income, which revealed that 18.8% of the sample were earning below the UK minimum wage, 19.1% were earning below the average UK wage, 14.3% approximately average UK wage, 10.2% above the average UK wage, and the rest (37.6%) earned considerably above the average UK wage. T-test comparisons between those who reported parents with behavioural addictions to those who did not report parental addictions, no significant differences were found between the groups in any of the above biographic details.
Measures
Demographic Questionnaire
This questionnaire included general background questions about participants such as age, gender, ethnicity, household income and marital status.
Parental Addiction
Participants were asked: “looking back at your childhood, do you think that your parent/s had an addiction to any of the following (please tick all appropriate answers)” and were given the following options: gambling, shopping, sex/pornography, work, exercise, screens (computer, TV, Phone), relationship or food (under/over). Options also included alcohol and substance addictions. For each of these participants were asked to choose between the options “yes”, “no” or “maybe”. For the purposes of the current study, only responses of “yes” were considered as a report of parental addiction.
Family Member Impact Questionnaire (FMI; Orford et al., 2005)
The FMI was used to measure the level of disruption to the family environment. This 16-item questionnaire was originally designed to reflect the harmful impact (stress) that drinking or drug–taking of a family member has on other family members or the family as a whole. We adjusted the wording of the questionnaire and the instructions in order to adapt allow participants to reply without making references to a particular addiction. In terms of instructions, we replaced the original instructions, which make reference to the last three months and to drinking/drug use with instructions that asked participants to note if, to their knowledge, any of the items occurred in their childhood. We changed the wording on some of the items, replacing “relative” with “parent/s” and in items 9, 13, 14 and 16 the term “drinking/drug use” was replace by the general term “behaviour”. Participants were asked to rate statements (e.g. “Did your parent/s have changeable moods?”, “Has your parent/s been late on unreliable?”) on a Likert scale ranging from 0 = not at all to 3 = often. An overall sum score was used to reflect the general impact of the behaviour on the family. In previous studies (Chan et al., 2016) the questionnaire revealed an internal consistency of α = .82–.85. In the current sample, Cronbach’s alpha was .90.
Severity of Dependence Scale (SDS; Gossop et al., 1995)
The SDS was used to measure substance and behaviour dependence. The original SDS is a 5–item questionnaire that provides a score indicating the severity of dependence on drugs. Items refer to the extent to which participants feel that: (a) their drug use is out of control (b) not taking the drug will cause worry/anxiety, (c) they worry about their drug use, (d) they wish they could stop, (e) they think it will be difficult to stop. Each of the five items is scored on a 4–point scale (from 0 = never/almost never to 3 = always/almost always). The total score is obtained through the additions of the five ratings with higher scores reflecting higher levels of dependence. In order to adapt this questionnaire to a range of substance and behavioural addictions we used a general term of “the following behaviours” followed by a list of behaviours: being online (email, text, twitter), exercising, over/under eating, drinking alcohol, using drugs, relationships, work, gambling. In the original study (Gossop et al., 1995) the questionnaire revealed an internal consistency of between 0.8–0.9 and in our study, Cronbach’s alpha values for each behaviour was as follows: being online .85, exercising .66, over/under eating .90, drinking alcohol .91, using drugs .90, relationships .85, work .80, and gambling .78. The internal consistency of all the behavioural addiction items together was .86 and for alcohol and .90 for drugs.
Symptoms Rating Test (SRT; Kellner & Sheffield, 1973)
The SRT was used to measure participants’ mental health. This measure is a symptom checklist that assesses the extent of mild to moderate physical and psychological ill health. Respondents rate whether they have experienced each of 30 symptoms in the last 3 months on a scoring scale of 0 = never to 2 = often. For the current study, only the 17 items in the psychological factor were used and the overall score was the sum of these items. The original authors (Kellner & Sheffield, 1973) did not report internal consistency figures but did report high levels of test–rest reliability and validity indicators. In the current study the Cronbach’s alpha for this scale was .93.
Connor–Davidson Resilience Scale (CD–RISC, Connor & Davidson, 2003)
The CD–RISC is a 25–item scale measuring psychological resilience and ability to “bounce back” following adversity. Participants are asked to rate the extent to which statements (e.g., “I am able to adapt when changes occur”) apply to them on a Likert scale ranging from 0 = not true at all to 4 = true nearly all of the time. The original authors reported a Cronbach’s alpha of .89 and intraclass correlation coefficient of 0.87. Cronbach’s alpha in the current sample was 0.92.
Results
Study variables were examined for normality, homeodascity and linearity. Study variables were normally distributed, residuals appeared to be equally distributed and linearity was observed between the predicting and predicted variables. In order to examine Hypothesis 1 we performed a multiple analysis of variance (MANOVA) comparing those with reported parental substance and behavioural addictions to those without reported parental behavioural addictions while using reported parental substance addiction as a covariate.
As can be seen in Table 1, Hypothesis 1 and Hypothesis 2 were mostly supported as participants who reported having parents with behavioural addictions also reported significantly higher levels of substance and behaviour dependence psychological symptoms and family dysfunction than participants who reported parents with no addictions.
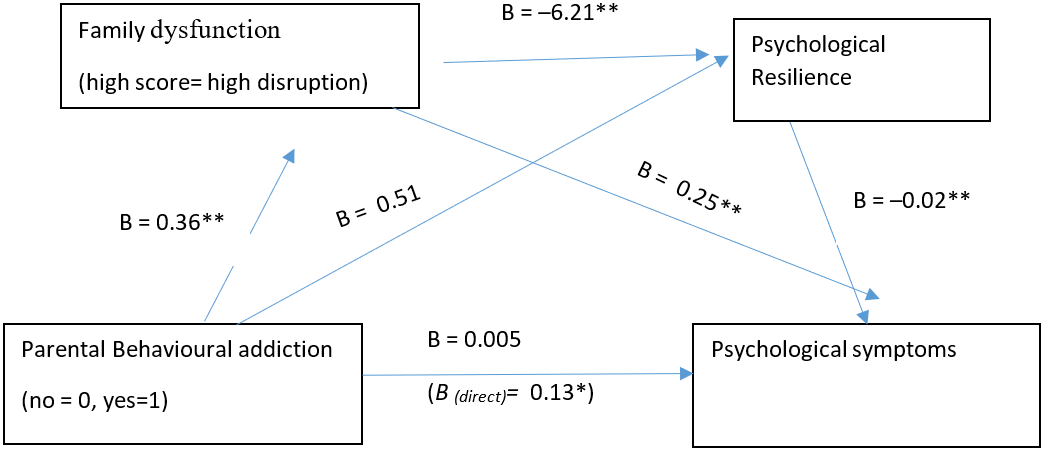
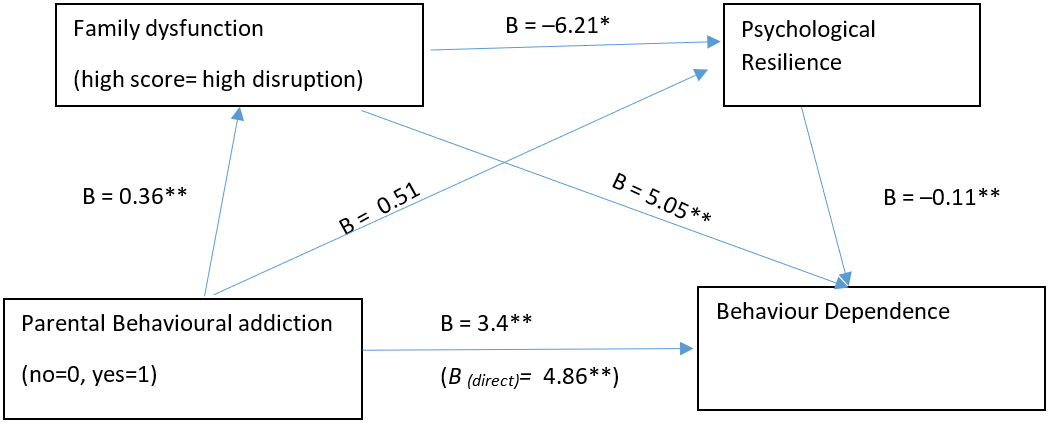
In Hypothesis 3 and 4 we predicted that the relationship between parental addictions and participants’ substance and behaviour dependency and mental health will be mediated by the participants’ level of family dysfunction and psychological resilience. We used Hayes’s SPSS process (Model 6) in order to test the potential moderation effects, while using reported parental substance addiction as a covariate. The results of these analyses appear in Model 1 and Model 2.


As can be seen in both Model 1 and Model 2, family dysfunction and psychological resilience mediate the relationship between parental behavioural addictions and psychological symptoms (full mediation) and participants’ own behaviour dependency (partial mediation). Thus, parental behavioural addiction are linked to more disruptive family environment (t(287) = 6.65, p < .001), which is linked to lower levels of psychological resilience (t(286) = –0.34, p = .74) which is linked to higher levels of symptoms t(285) = –11.83, p < .001) and participants’ behaviour dependency (t(285) = –3.12, p = .002). It was also found that a disruptive family environment is positively and significantly linked to psychological symptoms (t(285) = 7.20, p < .001) and participants’ own behaviour dependency (t(285) = 4.76, p < .001), thus mediating the relationship between parental behavioural addiction and these two outcomes. Psychological resilience did not emerge as having a significant independent mediating role as there does not seem to be a significant link between psychological resilience and parental behavioural addictions (t(286) = –0.34, p = .74).
When predicting participants’ substance dependency there was no significant link between participants’ substance dependency and a disruptive family environment (t(285)= 1.19, p = .24) or psychological resilience (t(285) = –1.10, p = .27), and so it seems that neither family environment nor psychological resilience play a role in the significant relationship between parental behaviour addictions and substance dependency during adulthood in this sample.
Discussion
In the current study we examined the role that a disruptive family environment and psychological resilience play in the relationship between parental behavioural addictions, as identified by participants, substance and behaviour dependency, and psychological symptoms. Corresponding to studies in the area of substance addictions (e.g., Arria et al., 2012; Biederman et al., 2000; Forrester & Harwin, 2006, 2008; Fraser et al., 2009; Hussong et al., 2005; Velleman & Templeton, 2016) we found that participants who grew up with parents with behavioural addictions were more likely to have higher levels of dependency on alcohol and drugs themselves and to have higher levels of psychological distress. The long-term negative impact of parental behavioural addictions found in our study highlights that while they may well be ‘invisible’, these addictions are just as disruptive and damaging to the family as substance addictions are and have a lasting impact on wellbeing. Our results reinforce previous calls (e.g., Engel et al., 2012; Manthorpe et al., 2018) to increase awareness and coverage given to behavioural addictions in clinical training and practice.
In line with previous studies on substance addictions (Barnard, 2007; Catalano et al., 2002; Keller et al., 2002), which found traumatic, unpredictable and chaotic family environments in families with parental substance addictions, we found that children of parents with behavioural addictions reported a more disruptive family environment than those who reported parents without such addiction.
Furthermore, our findings suggest that the impact of disruptive family environments on psychological distress and behaviour dependency in adulthood is partially due to the impact that the disruptive family environment has on the individual’s psychological resilience. While in the current study, parental behavioural addiction was not directly linked to psychological resilience, an indirect path of impact was found through a disruptive family environment. As noted earlier, psychological resilience is a multifactor construct related to an array of individual and psychosocial factors and in our study the environment shaped by the parental behavioural addiction led to decreased levels of psychological resilience, which were then linked to a less favourable mental health outcomes. This link between family dysfunction, psychological resilience and psychological symptoms (an indicator for participants’ mental health) is similar to findings in other areas (Leys et al., 2017). In the current context of behavioural addiction this link implies that involvement of services and interventions aimed at either improving the family functioning and/or increasing children’s levels of psychological resilience (see Park & Schepp, 2015; Ungar, 2015) may potentially reduce the long-term negative impact of parental behavioural addiction. Providing such interventions will initially require reversing the “invisibility” of behavioural addictions across the various social and addiction support services.
It should be noted that our study also implies that beyond a disruptive family environment and psychological resilience there may be other factors that are involved in the link between parental behavioural addictions and their children’s risk of developing their own behavioural and substance addictions. It may be that these are linked to genetic factors (Agrawal et al., 2016; Agrawal & Lynskey, 2008) or other psychosocial and parental factors (Velleman & Templeton, 2016). Future studies would do well to consider these factors and enhance our understanding of these additional pathways of impact.
Limitations and Recommendations for Future Research
The current study should be considered within its limitations. The study is cross–sectional and while mediation analysis may imply directionality, we cannot establish a direct cause and effect among any of our variables. Additionally, in the current study we have used a measure that assessed parental addiction and family environment based on participants’ retrospective subjective judgment (as opposed to more objective diagnostic tools), which can be prone to bias. Potential bias could have possibly been reduced to a certain extent if a more diagnostic tool based on a retrospective recall of specific behaviours were to be used (similar to the Severity of Dependence Test; Gossop et al., 1995 see Morsbach & Prinz, 2006 for details on increasing measures’ reliability); however, with the variety of addictions covered in this paper such a tool would have led to an impractically lengthy survey which in itself holds external and internal validity and reliability risks. It should also be noted that in their review Hardit and Rutter (2004) note that while there is evidently bias in retrospective ratings of the past, these tend to be false negative rather than false positive and while bias exists it is unlikely to be great enough to invalidate retroactive case control studies. Future studies may examine the immediate impact of parental behavioural addictions by including child participants rather than adults and longitudinal designs may be helpful in tracking the long-term impact of parental addictions without having to rely on retrospective reports.
In order to assess retrospective addiction related disruptive family dynamics in childhood, we had to make some adjustments to the instructions and some items on the Family Member Impact Questionnaire (FMI; Orford et al., 2005). These changes could have potentially impacted the validity and reliability of the measure; however, the internal consistency of the adjusted scale (Cronbach’s alpha of 0.90), which was in line with those found in previous studies, and its expected correlative relationship with parental substance addictions (r = 0.46, p < 0.001), parental behavioural addictions (r = 0.39, p < 0.001) and participants’ psychological symptoms (r = 0.44, p < 0.001) provide reassurance about the reliability and validity of this revised version.
Finally, an additional limitation stems from using an online survey which, as Johnson (2002) and Chiauzzi et al. (2013) note, often includes non–reprehensive self-selected samples, impacting on the ability to generalise the findings. And indeed, our sample included predominantly young white women. Nevertheless, we are also mindful of the recognised need to find a balance between methodology and the value of data (Chiauzzi et al., 2013) and believe that the findings in this study are of theoretical and practical value and that future research will be able to extend our findings to different social, cultural and gender groups.
Implications for Practice
With the above limitations in mind, this study suggests that the long-term impact that parental behavioural addictions have on children may be similar to that found in substance addictions. In addition, our results suggest that the path of this impact involves a disruptive family environment which reduces individuals’ psychological resilience which in turn results in less favourable psychological outcomes in adulthood. It therefore highlights the importance of addressing this long-term impact, possibly by providing interventions that address the disruptive family environment or increase children’s psychological resilience or both.
In terms of clinical implications, the current study suggests that more attention should be given by clinicians to behavioural addictions, which are many times invisible. The impacts of these addictions in a familial context seems to be as harmful and long lasting as other addictions and thus it is suggested that similarly to screening for substance addictions, behaviour patterns should also be examined, so that behavioural addictions can be detected, diagnosed and treated. Finally, the results also imply the need for early interventions with children of parents with behavioural addictions in order to reduce the risk of long-term impact on their mental health.